ASA PROPAGANDA
&
REBUTTAL
The American Society of Anesthesiologists (ASA) has made many claims over the years denigrating the 159 year profession of Nurse Anesthesiology. While more than 9 studies have demonstrated that there is no difference in outcome or quality of care, whether the anesthetic was delivered by Nurse Anesthesiologist or Physician Anesthesiologists, the ASA continues to make unsubstantiated claims, both through omission and fabrication. Below is an attempt to address and refute some of the more outlandish claims made by the ASA.
THE SILBER STUDY - 1992
ASA CLAIM
The Silber study examined the death rate, adverse occurrence rate, and failure rate of 5,972 Medicare patients undergoing two fairly low-risk procedures —elective cholecystectomy and transurethral prostatectomy.
[Silber, JH, Williams, SV, Krakauer, H, Schwartz, JS. “Hospital and Patient Characteristics Associated With Death After Surgery. A Study of Adverse Occurrence and Failure to Rescue.” Medical Care. 1992;30:615.]
Background: Anesthesia services for surgical procedures may or may not be personally performed or medically directed by anesthesiologists. This study compares the outcomes of surgical patients whose anesthesia care was personally performed or medically directed by an anesthesiologist with the outcomes of patients whose anesthesia care was not personally performed or medically directed by an anesthesiologist. The study was conducted using data obtained from Health Care Financing Administration (HCFA) claims records. The study group consisted of 217,440 Medicare patients distributed across 245 hospitals in Pennsylvania who underwent general surgical or orthopedic procedures between 1991-94. Dr. Silber headed a research team that included three anesthesiologists.
Conclusions: Both 30-day mortality rate and mortality rate after complications (failure-to-rescue) were lower when anesthesiologists directed anesthesia care. These results suggest that surgical outcomes in Medicare patients are associated with anesthesiologist direction, and may provide insight regarding potential approaches for improving surgical outcomes. (Key words: Anesthesiologists; anesthesia care team; quality of care; mortality; failure-to-rescue; complication; Medicare; general surgery; orthopedics.)
KEY EXERTS FROM THE STUDY:
1) This pilot project examined ideas that, to our knowledge, have not been examined previously, and more work is needed before the full significance of the results can be determined. It is especially appropriate, therefore, that the limitations of the project be recognized.
2) In his analysis of the Silber study, Dr. Michael Pine (physician and expert in quality and health care) stated that:
"Thus, the presence of board-certified anesthesiologists does not appear to lower the rate of complications, either alone or in combination with other factors such as high technology. It is not anesthesia care but the failure to rescue patients once complications occur which contributes to the death rate. On the other hand, unmeasured factors such as a higher percentage of other board-certified physicians in the hospital, also may account for the better outcomes."
3) Significantly, the Independent Regulatory Review Commission (IRRC), a Pennsylvania oversight commission that reviews health care proposals, carefully evaluated the Silber study, and issued a report rejecting the study as any basis for requiring anesthesiologist supervision of CRNAs.
4) This study Does Not “Compare Anesthesiologists Versus Nurse Anesthetists”
According to Dr. Longnecker, one of the anesthesiologist researchers: “The study ... does not explore the role of (nurse anesthetists) in anesthesia practice, nor does it compare anesthesiologists versus nurse anesthetists. Rather, it explores whether anesthesiologists provide value to the delivery of anesthesia care.” [Source: Memorandum from Dr. Longnecker to Certified Registered Nurse Anesthetists in University of Pennsylvania Health System’s Department of Anesthesia, October 5, 1998.]
REBUTTAL
Anesthesia safety was not the intent of the study and it was never about providers and mortality. It was done in ONE state (PA) and was about something totally different. The original authors required the ASA to change the name for their "massaged" study and the ASA shopped over 20 journals who all refused to publish it because of its glaring inaccuracies and frankly non-existent science.
This study DID NOT EXAMINE the safety record of any CRNA personally performing the anesthesia. The study, therefore, had nothing to do with CRNAs and did not compare the outcomes of care between nurse anesthesiologists and physician anesthesiologists.
The Silber study was a pilot study, i.e. a study to demonstrate the feasibility of performing a more definitive study concerning patients developing medical complications following surgery. It would be inappropriate to formulate public policy based on the Silber study; the study does not address CRNAs, and cannot be considered conclusive even about the issues that it does address.
This study’s conclusions support the proposition that certain facilities may benefit from having a board-certified anesthesiologist in the Intensive Care Unit. This may result in the “rescue” of some patients who have undergone elective cholecystectomies and transurethral prostatectomies and developed life-threatening postoperative complications.
The Silber study’s conclusions have nothing to do with nurse anesthesiologists or the nature of who may supervise, direct, or collaborate with nurse anesthesiologists. The study, however, did not involve examination of the outcomes of anesthesia in the operating room.
Hence, the conclusion to be drawn from this study is that, although the presence of a board-certified anesthesiologists may not make a difference in the operating room, it may make a difference in the failure to rescue patients from death or adverse occurrences after postoperative complications have arisen.
The IRRC stated that:
Based on our review of the 1992 Medical Care article, we have concluded, as its
authors clearly state, it is a preliminary study
and that caution should be taken in making any definitive conclusions. More importantly,
the authors did not consider the scenario of an operating physician delegating the administration of anesthesia to a CRNA, or what expertise the operating physician should have in order to safely delegate anesthesia to a
CRNA.
Therefore, we do not believe this study should be used
as justification for the significant change in practice for the administration of anesthesia.
The IRRC further stated that:
There have been
two studies, both completed over 20 years
ago, that compared the outcomes of anesthesia services provided by a nurse anesthetist and an anesthesiologist.
Neither
of these studies concluded that there was any statistically significant difference in outcomes between the two providers.
This conclusion was also reached by the Minnesota Department
of Health, which recently completed a study on the provision
of anesthesia services. In fact, most studies on anesthesia
care have shown that adverse outcomes and deaths
resulting from anesthesia has decreased significantly in the
last several decades as [a] result of improved drugs and monitoring technology.
Why, then, was such a misleading title (“Do Nurse Anesthetists Need Medical Direction by Anesthesiologists?”) chosen for the abstract?
The answer: for political reasons. Consider these facts:
• The abstract was published in the midst of the controversy between anesthesiologists and nurse anesthetists over HCFA’s proposal to remove the physician supervision requirement for nurse anesthetists in Medicare cases 2000.
• The study was funded in part by a grant from the American Board of Anesthesiology, which is affiliated with the ASA. ASA vehemently opposes HCFA’s proposal.
Why was the name of the abstract changed prior to publication of the paper in the July 2000 issue of Anesthesiology? Most likely for the following reasons:
• As Dr. Longnecker stated in his memorandum, the study was not intended to examine the question posed by the abstract’s title.
• The study clearly could not and did not answer the question posed by the abstract’s title.
• Pressure from AANA in the form of statements to the media and commentary published on the internet forced the researchers and ASA to rename the paper for publication.
ASA CLAIM
Physician Anesthesiologists Keep Your Constituents Safe
There’s a good reason why 93% of surgeons and nearly 90% of patients want physician anesthesiologists in the operating room to respond with their lifesaving expertise in critical moments:* As the only medical doctors on the Anesthesia Care Team, physician anesthesiologists are uniquely qualified to prevent complications and respond to emergencies. They are responsible for the safe provision of anesthesia, and as experts in perioperative care, they also identify, minimize, and prepare for potential risks before surgery and help direct patient recovery and pain management after the procedure.
Physician anesthesiologists’ education and training are unmatched on the Anesthesia Care Team. That’s why they lead the team and take charge of patient safety. You were elected to represent your constituents and fight for their best interests. Make sure your constituents are protected by keeping physician anesthesiologists involved in all phases of anesthesia care.
*Source: Independent survey conducted by PSB for the American Society of Anesthesiologists in December 2019.
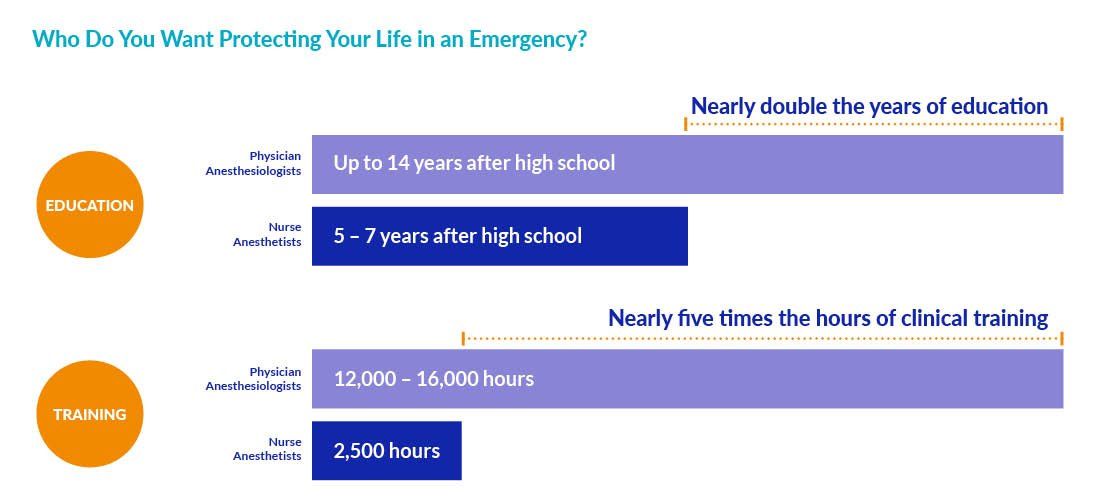
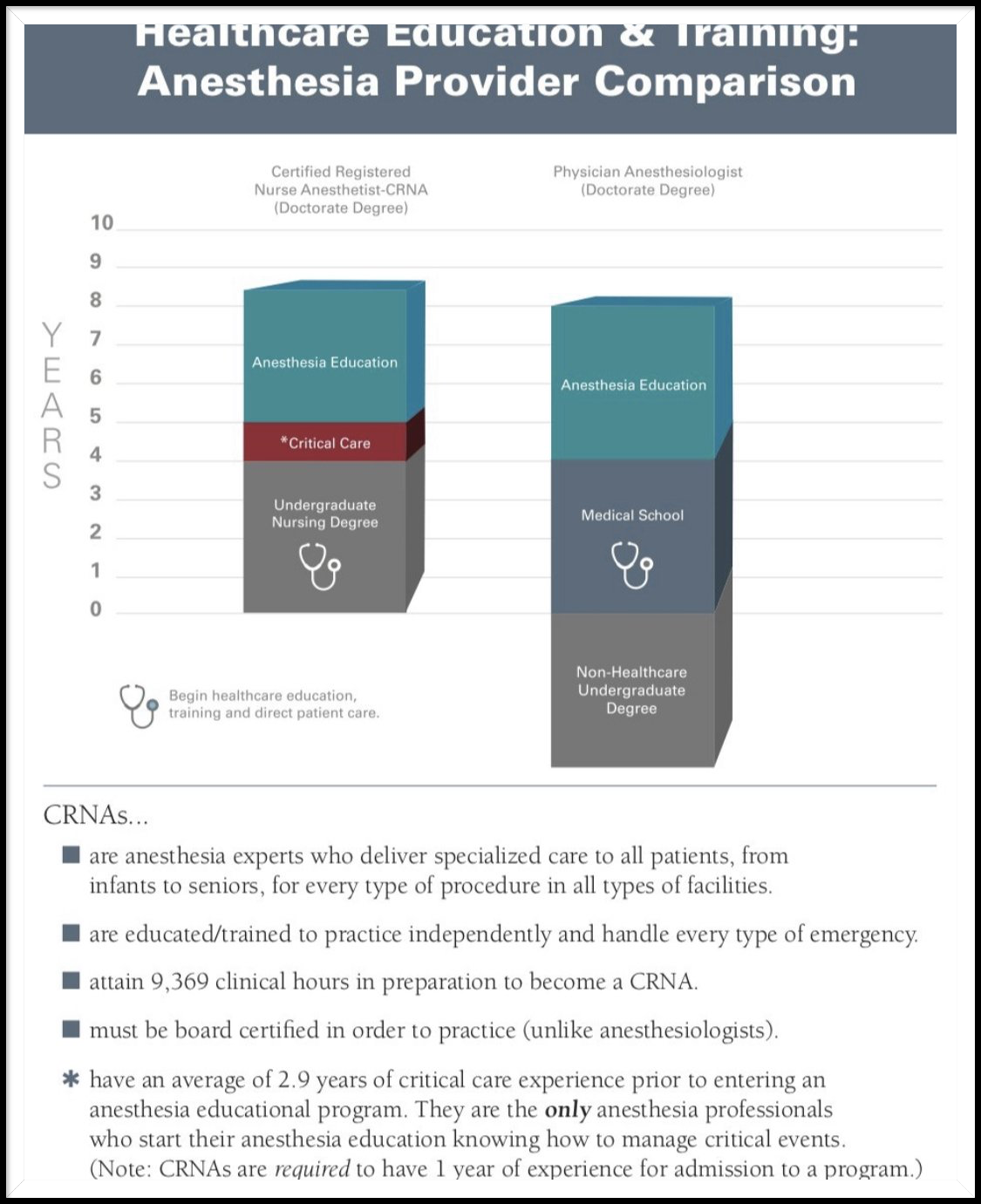
Misleading and not reflective of the facts regarding the education of CRNAs - which in many instances is superior to the education of a physician anesthesiologist.
1) 2-3 years of hands-on Intensive Care and/or Trauma clinical experience handling the most challenging patients in healthcare.
2) Roughly 10,000 hours in preparation and training to become a CRNA.
3) CRNAs are the only provider to have clinical hands-on critical care experience prior to setting foot in an operating room during their residency - bringing a significant level of healthcare experience above and beyond the typical physician enter medical school.
REBUTTAL
Unfortunately, the ASA refuses to produce the details pertinent to this survey for obvious reasons - which is inherently bias. The reality is, when a surgeon, nurse, or their family members need an anesthetic, more than 95% of the time they will request a CRNA NOT and MDA. Why? Because CRNAs are the only anesthesia provider to actually provide 100% of their own hands-on anesthetics in more 80% of the ~52 million anesthetics performed annually. The relationships CRNAs build through daily interaction with surgeon and nurse colleagues cultivate and environment of trust and confidence in the abilities that CRNAs bring to the surgical and procedural areas. This is a study that the ASA would never undertake because they know it would completely undermine their agenda to malign CRNAs at every opportunity. If safety were an issue, does anyone believe CRNAs would still be INDEPENDENTLY provide millions of anesthetics every year? Since the civil war, CRNAs have personally delivered more than 1.4 billion anesthetics safely and with the highest quality of care.
ASA CLAIM
The presence of a physician anesthesiologist prevented 6.9 excess deaths per 1,000 cases in which an anesthesia-related or surgical complication occurred.*
REBUTTAL
Once again, the ASA is attempting to use this is a twenty-year old study (Silber Study 1992) led by a physician anesthesiologist and ASA member. In the study, they used 8x the number of medical directed cases and used a 30-day death rate after
admission, and in-hospital complication rate and then defined the failure-to-rescue rate as death after complications "in which anesthesia-related.
Nearly two years later, the Pennsylvania study was published in the July 2000 issue of Anesthesiology with the title, “Anesthesiologist Direction and Patient Outcomes.”
Both the Journal of the American Medical Association and
the New England Journal of Medicine declined to publish the Pennsylvania study, forcing the ASA to publish the study in its own journal if it wanted the study to be published at all.
